Vertigo can be very uncomfortable and quite scary. If you suffer from chronic dizziness and are continually told by your doctor that it is BPPV and just given medications, the most important thing to understand is that proper testing is essential.
The most common diagnosis that is given when a patient reports having dizziness or vertigo to their doctor is BPPV or benign paroxysmal positional vertigo. Your doctor usually will say something like, “You have a crystal or rocks in your ear.” They will usually try to treat you by moving your head around a bit and then prescribing you an anti-histamine drug and usually an anti-cholinergic drug, such as meclizine or antivert. Anti-vertigo medications may be considered in acute, severe exacerbation of BPPV, but in most cases are not indicated and eventually can make the problem worse.
BPPV is the most common cause of vertigo but the symptoms of BPPV can mimic symptoms associated with a central brain based cause for vertigo. The cause must be determined via proper examination and advanced neurological testing.
Patients with BPPV will typically have vertigo symptoms when they tilt their head, roll over in bed, look up or under or make a sudden head motion.
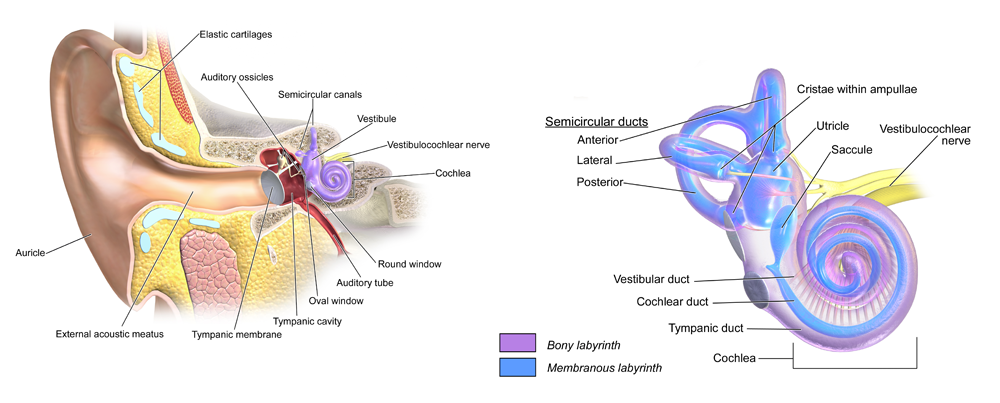
The vertigo associated with BPPV is caused by crystals disrupting the normal fluid dynamics in the semicircular canals of the inner ear. Within the inner ear lie collections of calcium crystals known as otoconia . In patients with BPPV, the otoconia are dislodged from their usual normal position within a part of the inner ear known as the utricle and migrate over time into one of the semicircular canals. When a person with these dislodged crystals moves their head relative to gravity, the gravity-dependent movement of the heavier otoconial debris within the affected semicircular canal causes abnormal (pathological) inner ear fluid displacement and a resultant sensation of severe rotational vertigo.
It’s unfortunate but many doctors are minimally trained in determining the variety of BPPV the patient is suffering from. There are three inner ear semicircular canals on each side of the head (posterior, anterior and horizontal). The otoconia crystals can get into any one of these canals on each side or a combination of multiple canals. Based on anatomical position, crystals are most commonly found in the posterior canal.
Because the posterior canal is the most common location, many doctors are minimally trained in all the canal diagnostic procedures and corrections for all the canals and typically rely on the posterior canal repositioning maneuver for everyone. If the maneuver is performed improperly or it is not the correct one for the canal(s) involved, it will be ineffective. In this case most doctors continue to prescribe Meclizine which is contraindicated for long term use. Meclizine is a vestibular sedative, and in the long run can decrease the brains ability to adapt to the problem thereby creating a chronic vertigo condition.
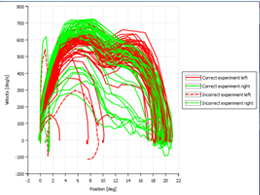
Each individual semicircular canal will cause a very specific variety and direction of a type of abnormal eye movement known as nystagmus. Nystagmus is a type of quick bouncing of the eye that is caused when there is an imbalance in how the brain or inner ear is functioning from side to side. Careful examination of what direction the nystagmus is beating will let us know what specific canal is involved and the exact positional maneuver that is indicated.
We use VNG (video nystagmography) goggles to determine the variety of BPPV or some other neurological problem that is causing our patient’s vertigo. The VNG will pinpoint the quality and direction of the eye nystagmus. It can also be used to retest the patient to see if the otoconia debris has been fully repositioned and emovedafter the proper maneuver is performed.
 The other critical aspect to helping patients overcome BPPV is to fully rehabilitate weak brain areas so they calibrate to the new inputs from a balanced inner ear that does not have crystals within the canal.
The other critical aspect to helping patients overcome BPPV is to fully rehabilitate weak brain areas so they calibrate to the new inputs from a balanced inner ear that does not have crystals within the canal.
After having BPPV and then having the crystal repositioned and eliminated the brain must then recalibrate to the new normal. The cerebellum is the area of the brain that recalibrates and makes adjustments to alterations in inner ear input. We do specific cerebellar and brain rehabilitative exercise to improve function in these areas. This rehabilitation is essential for a full recovery especially in those with a combination of BPPV and age-related cerebellar functional decline. The specific areas of the brain that need to be rehabilitated through exercise are determined using advanced neurological testing.
If you suffer from chronic dizziness and are continually told by your doctor that it is BPPV and just given medications, the most important thing to understand is that proper testing is essential. In order to help a patient suffering from positional vertigo the doctor must use advanced neurological testing to determine the quality and direction of the nystagmus. Many times it is revealed that the patient does not have BPPV at all and that their dizziness problem is from another neurological problem all together. Many times it is revealed that the BPPV is in multiple canals or a less common variant. In this case the traditional Eply’s repositioning maneuver will not work. If this sounds like you please do not hesitate to call our office to set up an initial vertigo evaluation.